1.Introduction
Attracting and retaining skilled psychiatric nurses in forensic and correctional environments presents a significant challenge, exacerbated by the ongoing nursing shortage and lack of attention to these unique nursing specialties. Many potential candidates are unaware of the critical and rewarding roles these nurses play in managing complex health conditions and psychiatric disorders[1] because academic preparation and on-site training are not typically available at their colleges.[2] Consequently, as health problems continue to escalate for people dealing with the criminal justice system,[3] whether they are incarcerated, victims of crimes, or otherwise entangled, the shortage of nurses prepared to help these individuals has become a national crisis.[4]
Forensic nurses may focus on caring for individuals who have experienced criminal acts such as assault, rape, trafficking, abuse, neglect, bullying, harassment, theft, or any act that has traumatized them, including the trauma to or death of a loved one. They may assist medical examiners in their work, including conducting autopsies, and assist legal teams and law enforcement with evidence collection and providing testimony in court. Conducting psychiatric assessments and treatment may also be a critical aspect of their work. Nurses who specialize in correctional settings also work with vulnerable populations. What may be perceived as “unpredictable” behavior among incarcerated individuals is often untreated mental illness, seven times more prevalent in prison populations than in the general public.[5] Correctional nurses, like their forensic counterparts, need special training in the assessment of mental health as well as substance use. They should also be well-versed in trauma-informed care, as they may need to advocate/care for individuals who attempt suicide, are victims of assault, and have psychiatric crises.
2.Method
This study utilized an integrative review methodology to synthesize diverse empirical and non-empirical evidence related to correctional and forensic psychiatric nursing. The literature review was conducted using PubMed, MEDLINE, APA PsycINFO, and CINAHL Ultimate. The focus of this search was to find evidence on the current status of nurses working as specialists in correctional and forensic settings, the implications of shortages in these areas, and to identify potential solutions. Only phrases such as “nurse shortages” AND “corrections” AND “forensics” AND “psychiatric and/or mental health settings” AND “behavioral health settings” were used in the search for nursing deficits. These terms, alone, provided evidence of shortages and their implications. However, to find models of nursing colleges partnering with these institutions to train nurses, the authors used phrases such as “peer-reviewed article” AND “collaborations between academic and correctional institutions to train nurses.” The limited number of articles in this particular area was thoroughly reviewed, and article references were consulted for additional relevant information. Inclusion criteria consisted of peer-reviewed English-language articles published between 2018 and 2025. Exclusions included dissertations and letters, as well as settings outside the United States (see Figure 1).
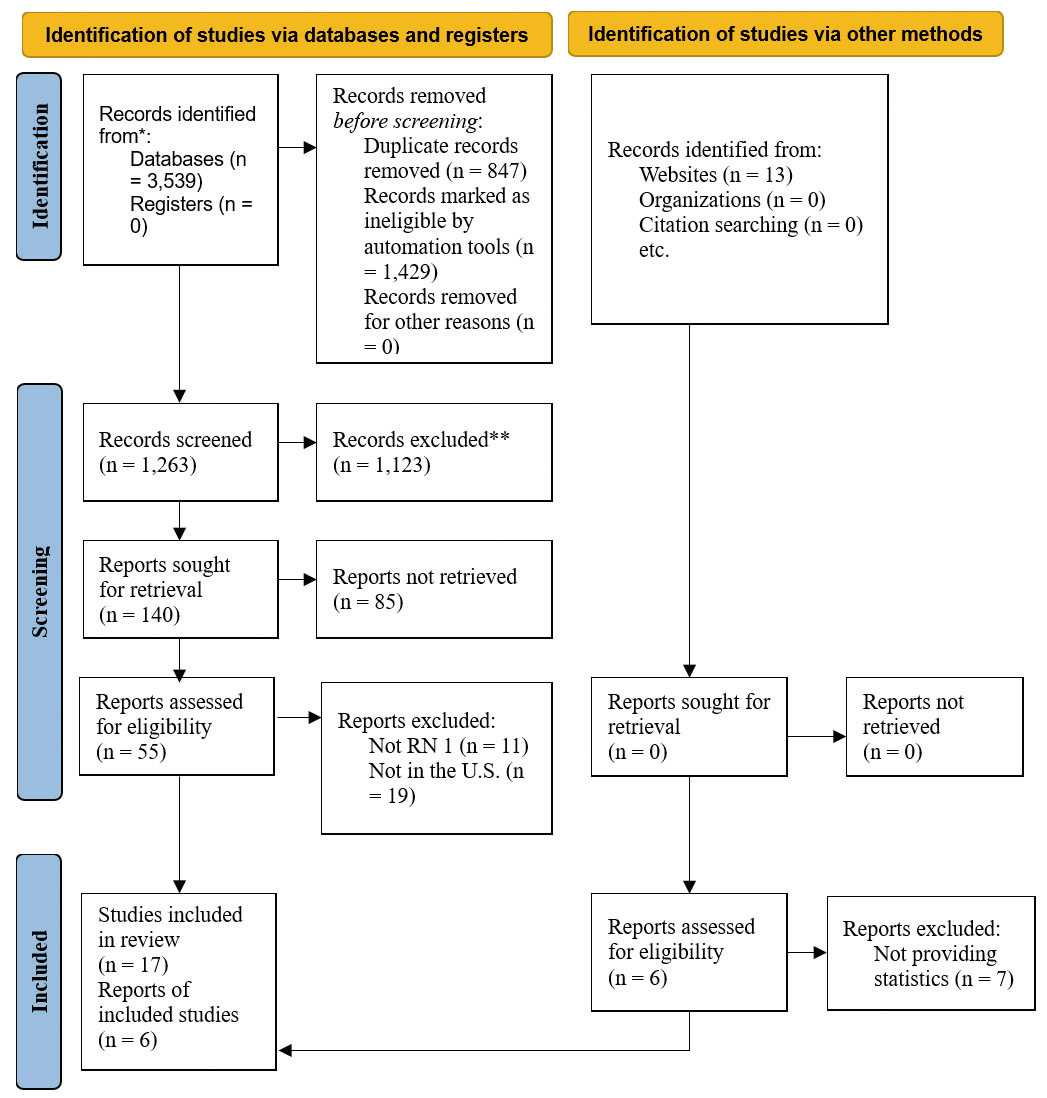
Figure 1.
PRISMA flow diagram
3.Results
The literature search revealed a limited number of articles addressing the shortage of correctional and forensic psychiatric nurses and the rewards of a career in these specialties. However, it did indicate a history of nursing shortages in these areas and the escalating need to address current deficits.[1, 3] Moreover, the shortages applied not only to correctional and forensic venues but to psychiatric health settings in general.[6] The following evidence provides a snapshot of the evolution of these specialties and expands on ongoing challenges, including the consequences of nursing vacancies and their implications for nursing education.
3.1Early advocates for nursing in psychiatric, forensic and correctional settings
Throughout history and despite many challenges, psychiatric nurses have played a pivotal role in shaping the healthcare system. Pioneers such as Dorothea Dix emerged as a recognized force between 1840 and 1887, due to her dedication to caring for the mentally ill and advocating for humane treatment of individuals in correctional settings.[7] Recognized for developing the theory of interpersonal relations in 1952, Hildegard Peplau provided psychiatric nurses with a theoretical foundation and skills to enhance their interactions and level of engagement with patients.[8] Recognized in 1975 as a pioneer in correctional nursing in New York, Rena Murtha’s work cultivated the beginnings of a structured, safe, and visible nursing profession within the prison system.[9] In the 1990s, Virginia A. Lynch developed the integrated practice model, which bridged the gap between nursing practice, forensic science, and the criminal justice system. With her focus of caring for forensic patients, Lynch’s conceptual model was pivotal in establishing this specialty, but the model was barely recognized until it was endorsed by the American Academy of Forensic Sciences in 1991.[10] These pioneers undoubtedly broadened and advanced the scope of professional nursing, overcoming many challenges along the way. However despite theirs and many others’ efforts a long history of stigma and misconceptions has persisted adversely affecting perceptions of these specialties, rather than lauding them with the recognition and respect they deserve.[4]
3.2The effect of persistent stigma about careers in correctional, forensic, and psychiatric healthcare settings
Despite the strong influence of nurses in decreasing stigma and dehumanizing attitudes toward incarcerated individuals who suffer from psychiatric disorders and/or substance use,[11] the limited amount of peer-reviewed literature endorsing a career in correctional nursing may reflect a continuing perception problem.[12] In fact, psychiatric nursing, in all its settings, continues to bear the weight of stigma perpetuated by ignorance and misconceptions about mental illness, even among some nursing professionals.[13] Even at schools where psychiatric mental health nursing specialties are offered, this career choice has had a rocky past. Nurses were often isolated, compartmentalized, or marginalized depending on their environments. For example, the “psych ward” was often separated from the rest of the facility, and nurses had to traverse a long hallway to reach a locked unit considered the “dreaded” clinical rotation.[13] The strain between nursing care and custody is a unique factor among correctional, and in some cases, psychiatric facilities in which the main focus of safety and security often overrides care-focused goals. This may leave little room for building rapport with patients and delivering care that adequately addresses patients’ needs.[12] Furthermore, concerns of safety among new hires or those in training may pose a barrier with efforts to comply with the American Nurses Association (ANA) standards for delivering exceptional care to patients with mental health issues in correctional settings.[4]
In fact, recruitment of psychiatric mental health nurses continues to be a major challenge, with personal safety at the forefront of potential hires’ concerns.[14] However, the fear for one’s safety with these patients may be significantly allayed with understanding that many of them have a history of trauma. Sufficient training in trauma informed care (e.g., acknowledging the trauma, building trust and identifying behavioral triggers, collaborating on behavior plans, maintaining professional boundaries), can help deter behaviors that threaten safety.[15]
Unfortunately, misconceptions also abound regarding the reputation of nursing careers in correctional or forensic psychiatry. In a Texas psychiatry residency study (N = 44) and in surveys of 134 Canadian psychiatry residents, Morris and West (2020)[16] learned that these psychiatric mental health professionals had stigma-laden perceptions about careers in corrections:
Incarcerated patients are less deserving of mental health care than other patients.
Working in correctional psychiatry supports mass incarceration.
Correctional psychiatry is more dangerous than practicing psychiatry elsewhere.
Correctional psychiatry is a less respectable subspecialty. There are few teaching opportunities in correctional psychiatry.
There are a few research opportunities in correctional psychiatry. (p. 251)
These misconceptions must be unearthed and discussed early in health professions students’ courses, especially with the critical demand for psychiatric professionals in our prisons, justice system, and inpatient mental health facilities.
3.3Mental illness and the current need for nursing specialties
According to the 2016 Survey of Prison Inmates, approximately 43% of state and 23% of federal prisoners reported a need for psychiatric services. Conversely, national nursing workforce data collected in 2018 revealed that only 13,775 nurses worked in correctional facilities, comprising only 0.5% of all registered nurses.[17] In their Special Report about psychiatric health problems of U.S. inmates, Bronson and Berzofsky[18] found that approximately 40% of incarcerated individuals experienced serious psychological distress. This percentage was supported by findings from the National Alliance for Mental Illness (NAMI)[19] which reported that 37% of incarcerated individuals in state and federal prisons had mental illness, and that 44% in jails across the country. According to NAMI (2025),[19] 63% of incarcerated people with a history of mental illness did not receive treatment.
3.4Consequences of nursing vacancies
Although the need for psychiatric care in correctional facilities in the U.S. is at a critical point, a 2018 survey of six states reported encountering 85% hardships in hiring nurses and other psychiatric health professionals to fill these positions.[16] Significant nursing vacancies are likely to compromise the level and degree of nurses’ efforts to adhere to ANA standards, particularly for patients with mental illnesses. For example, the fewer nurses serve in these settings, the less time and opportunity they have for mentoring new hires about the parameters of their correctional nursing roles. This ripple effect from shortages impedes the diligence necessary to identify and address mental health concerns, resulting in delays in triage and prompt communication with the medical team when patients’ needs (e.g., psychiatric disorders, trauma-related behavioral problems) extend beyond registered nurses’ scope of practice and require specialized psychiatric nursing care. The shortage of nurses limits opportunities for effective, personalized communication, hindering patients’ engagement and interest in learning about their medical conditions. Ultimately, this compromises their ability to understand, let alone participate, in managing their health collaboratively.[20,21,22,23]
Limitations of nursing presence in a facility can also impede collaboration with correctional officers, making it more challenging for patients to receive timely, critical medical care. This includes care for patients diagnosed with serious psychiatric illnesses.[20] Increasing the number of well-trained nurses in these specialties and settings would foster teamwork and enhance promotion of health equity on several fronts: more time to build rapport and trust with patients and correctional officers, opportunities to model and support enhanced collaborative practices (e.g., problem-solving, decision-making, arriving at consensus), promote healthier behavioral practices from patients with mental health issues, and contribute to the reduction of recidivism.[24] For example, psychiatric nurses specializing in corrections can help patients transition to parole status or full release by ensuring stabilization of mental illnesses symptoms and associated behaviors (including substance addictions), increased health literacy, a variety of resources to access that are tailored to their needs (especially community mental health centers), cognitive–behavioral interventions that foster adherence to medication regimes, and problem-solving skills to aid in communal living, such as heightened recognition of their mental, emotional, and behavioral “triggers” (e.g., particular stressors or activating stimuli), including a safe plan to execute if they are triggered.[25] In a multistate sample of formerly incarcerated men (N = 871), researchers found that the men who made improvements in mental health while still in prison were associated with reductions in recidivism[24, 21, 22, 26] (e.g., see the Appendix).
4.Discussion
Just as many incarcerated individuals need psychiatric care so do the individuals whose lives have been altered by contact or connection with them. These individuals may have experienced violence, trauma, abuse, neglect, trafficking, and/or mental disorders linked to the legal or criminal justice system. Whether it means caring for populations in our prisons and jails, in detention centers community-led programs, or victims, family members, coworkers, or others, nursing students must first know that these careers exist. Then they must have opportunities to explore them, and be trained to succeed in them.
4.1Benefits of careers in correctional or forensic nursing
Nurses need to know about the variety of career opportunities in correctional or forensic settings, each offering different levels of patient care. These roles can focus on education, primary care, acute, emergent, and chronic care, and on mental and behavioral health.[27] Forensic nurses may focus on individuals who have experienced trauma from violence. Benefits of these nursing specialties typically include professional growth across a variety of sectors, offering new graduates a better-than-average chance of being hired and maintaining job stability, given the high demand. Competitive pay and benefits are also part of the package. For most nurses who do not want to lose sight of why they got into nursing in the first place, they will have opportunities to make positive impacts that ripples out to the general population in myriad ways.[28]
4.2Creating partnerships with academic institutions to develop specialties
Creating partnerships with academic institutions to introduce these specialties would enhance the implementation of evidence-based practice, provide up-to-date information, professional development, and ultimately better preparing nurses for a more productive start and career longevity in these arenas.[2, 29] To help new hires have a positive experience entering these settings, training in areas such as applying emotional intelligence to safely interact with various types of patients, simulations to ensure competency in skills, and purposeful, topic-driven collaboration with security officers and correctional staff should be mandated as part of orientation.[30] The roles of nurses in these fields and at each particular institution should also be investigated and discussed, as some settings lack defined role parameters, which can shake confidence or hamper nurses’ professional identity.
Depending on the areas of most need, university programs and various forensic nursing settings can partner to encourage more nurses to consider a career in this area. For example, if even one mental health nursing course was devoted to caring for people who have experienced trauma, course instructors could establish partnerships with a number of local facilities (e.g., juvenile detention centers, legal firms, psychiatric facilities that work mainly with the justice system) for students to visit, shadow nurses there, and attend debriefs, so they can ask questions about the pros and cons of the job. These partnerships could include having students in nursing education and mental health programs develop guides or manuals for correctional officers to help them better deal with the mental health issues of patients in these settings. Students could go as a group to present their guide, receive feedback from correctional officers and other personnel, and learn about the world of corrections.[2, 26, 29]
4.3Incorporating a correctional and forensic specialty: Highlights
Incorporating forensic and correctional nursing education into academic nursing programs is essential to prepare nurses for the unique challenges of working in these environments. Shelton et al. (2020)[4] emphasized the importance of professional socialization into correctional nursing, noting that many nurses are not adequately prepared for the complexities of this specialty. Although the literature about residency programs tailored explicitly to psychiatric nurses is limited, a program structure offers a favorable outlook for new graduates.[31] Clifton et al. (2022)[2] advocated academic-practice partnerships within justice systems, demonstrating how collaboration can enhance educational outcomes and workforce readiness. Offering continuing education focused on mental health assessments, substance use disorders, and evidence-based interventions is vital for supporting nurses in these roles. Keller et al. (2022)[27] found that correctional nursing environments are often marked by stressors such as workforce violence and lack of organizational support, which can lead to burnout. Addressing these challenges through curriculum and policy is crucial for sustaining a healthy workforce. In addition, other experts have advocated for initiatives that strengthen the skills and resources of justice health professionals, highlighting the importance of delivering care in correctional environments grounded in empirical evidence.[32] With respect to garnering attention, Jones-Vanderleest and Roose-Goldstein (2025)[33] demonstrated that jail-based rotations can promote interest in correctional healthcare careers, suggesting that experiential learning is a powerful tool for recruitment and retention.
Establishing effective academic-practice partnerships between nursing colleges and correctional/justice systems is the foundation upon which these nursing specialties can be launched and maintained. In their pioneering work, Clifton et al. (2022)[2] offered four examples of academic-practice partnerships (APPs) and factors that aided their development.[29] In the first, an APP between the nursing college and the Department of Corrections had to be reviewed and receive Institutional Review Board approval, which meant that both parties had met numerous times to listen to each other’s needs and expectations. Funding had to be explored, such as in-kind contributions from faculty. This was addressed by offering a nurse clinician free educational courses in exchange for services to nursing students who opted to participate in an intervention that focused on helping incarcerated individuals to learn self-care management strategies. In their second APP with Juvenile Justice, the key lessons were that it was often highly challenging to work with other professionals whose priorities may be different, that there are multiple opportunities for personal growth, students universally believe the work is personally and professionally worth it, and students believe that they can and do have an impact.[2] The third APP established was research-oriented. In this partnership, the primary goal was to improve the “health of and the health care provided to people living in prison”[2] (p. 25). In the last APP, a spiritual community and “jail partner” were the double foci of investigation and collaboration. Overall, this multi-layered four-part APP found convincing evidence that students’ impact on the correctional environment was positive and important. Students had increased compassion for these patients and less stigma-related perceptions of them.
At another school of nursing, Shelton et al. (2020)[4] recognized that there was a growing interest in correctional nursing and that supporting students who wanted to explore this career or supporting nurses already involved in it might be aided by continuing-education credit, would be on areas where the need was greatest: assessment/treatment of psychiatric and substance use disorders, the withdrawal process, suicide risk, and evidence-based interventions. This group divided their professional development curricula into two main content areas per students’ experience: novice nurses newly entering correctional systems and experienced nurses new to corrections.[21] The primary goal was to offer a curriculum that would build a competent correctional nursing workforce. These examples of how nursing schools are addressing a profound curricular gap in equitable healthcare in corrections illustrates that the field of nursing is well-positioned to develop these specialties.
5.Conclusion
The need for more nurses in forensic and correctional settings is not new. Recently, however, this need has become critical as the volume of people in these settings increases alongside growing nursing vacancies. As with any large, important project affecting healthcare at the national level, the solution will require vision, leadership, strategic planning, and the collaborative efforts of multiple stakeholders. The solution begins with piloting programs that first partner with the facilities and institutions that will hire nurses with these specialties. In collaboration, these nursing specialties will develop programs that address their needs. Students will be invited to experience these environments and meet the people they would work with and serve. They would also have the opportunity to bring their own perceptions, including ones influenced by stigma or myths, to the table. However, building the kind of trust and respect between partners that is called for in these settings will necessitate further research to develop strong academic programs, including the use of simulation to help students prepare first in the safety of the academic environment. The next step would be to bridge students’ real-world knowledge gaps with half-day, full-day, week-long, and/or semester-long experiences in the setting, paired with mentors. Finally, inviting correctional, psychiatric, or forensic nurses who love their careers to share their professional experiences in academic settings might encourage students to consider the many career opportunities in these fields. These specialties are special, and they, like the populations they serve, can no longer be neglected.
Authors contributions
Ms. Monica Nebel and Dr. Veronica Decker contributed equally to all aspects of the work, including study design, literature review, synthesis of findings, manuscript writing, and critical revisions. The authors share equal responsibility and authorship. Both approved the final manuscript.
Funding
Not Applicable.
Conflicts of Interest Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Not Applicable.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
Not Applicable.
References
- Shelton D, Roscoe L, Kapetanovic T. The correctional nursing workforce crisis: An innovative solution to meet the challenge. Journal of Correctional Health Care. 2025;31(2):82-89. doi:10.1089/jchc.24.09.0079
- Clifton J, Maruca A, Loeb S. Nurse academic-practice partnerships in justice systems: Building upon the evidence. Journal of Professional Nursing. 2022:20-27. doi:10.1016/j.profnurs.2022.02.006
- Timmer A, Nowotny K. Mental illness and mental health care treatment among people with criminal justice involvement in the United States. Journal of Health Care for the Poor and Underserved. 2021;32(1):397-422. doi:10.1353/hpu.2021.0031
- Shelton D, Maruca A, Wright R. Nursing in the American justice system. Archives of Psychiatric Nursing. 2020;34(5):304-309. doi:10.1016/j.apnu.2020.07.019
- Gómez-Figueroa H, Camino-Proaño A. Mental and behavioral disorders in the prison context. Revista Espanola de Sanidad Penitenciaria. 2022;24(2):66-74. doi:10.18176/resp.00052
- Delaney K, Vanderhoef D. The psychiatric mental health advanced practice registered nurse workforce: Charting the future. Journal of the American Psychiatric Nurses Association. 2019;25(1):11-18. doi:10.1177/1078390318806571
- Strickler J, Farmer T. Dorothea Dix. Nursing. 2019;49(1):49-51. doi:10.1097/01.NURSE.0000549724.14939.d8
- Martinez A. Therapeutic alliance in mental health care. Nursing. 2021;51(10):56-60. doi:10.1097/01.NURSE.0000791764.52720.45
- American Nurses Association. Correctional Nursing Scope and Standards of Practice (Third ed.). American Nurses Association. 2020.
- Valentine J, Sekula L, Lynch V. Evolution of forensic nursing theory—Introduction of the constructed theory of forensic nursing care: A middle-range theory. Journal of Forensic Nursing. 2020;16(4):188-198. doi:10.1097/JFN.0000000000000287
- Reagan L, Kitt-Lewis E, Loeb S. Health equity for people living in correctional facilities: Addressing bias, stigma, and dehumanization. Research in Nursing & Health. 2024;47(4):359-365. doi:10.1002/nur.22405
- Dhaliwal K, Hirst S. Correctional nursing and transformational leadership. Nursing Forum. 2018;54(2):192-197. doi:10.1111/nuf.12314
- Soltis-Jarrett V. The future of psychiatric-mental health nursing: Observe, reflect, and take action to empower knowledge for the greater good. Issues in Mental Health Nursing. 2023;44(10):1071-1079. doi:10.1080/01612840.2023.2270066
- Ratnapradipa K, Houfek J, Gearhart P. Exploring the dynamics of attracting and retaining acute care psychiatric registered nurses: An in-depth analysis using focus groups. Journal of Nursing Management. 2024:1-11. doi:10.1155/2024/3167255
- Vincenti S, Grech P, Scerri J. Psychiatric hospital nurses’ attitudes towards trauma-informed care. Journal of Psychiatric and Mental Health Nursing. 2021;29(1):75-85. doi:10.1111/jpm.12747
- Morris N, West S. Misconceptions about working in correctional psychiatry. Journal of the American Academy of Psychiatry and the Law. 2020.
- National Academies of Science. The future of nursing 2020-2030: Charting a path to achieve health equity. The National Academies Press. 2021. doi:10.17226/25982
- Bronson J, Berzofsky M. Indicators of mental health problems reported by prisoners and jail inmates, 2011–12 (NCJ 250612). U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics. 2017. https://bjs.ojp.gov/content/pub/pdf/imhprpji1112.pdf
- National Alliance on Mental Illness. Mental health by the numbers|NAMI. NAMI. https://www.nami.org/about-mental-illness/mental-health-by-the-numbers/#::text=Millions
- Blair P. Health and safety in correctional facilities: A framework for action to overcome obstacles. Journal of Correctional Health Care. 2022;28(6):378-383. doi:10.1089/jchc.21.12.0138
- Lehrer D. Compassion in corrections: The struggle between security and health care. Journal of Correctional Health Care. 2021;27(2):81-84. doi:10.1089/jchc.20.07.0061
- Cukale-Matos S, Champion J. Exploring cognitive dissonance in the correctional nursing experience. Public Health Nursing. 2021;39(3):545-552. doi:10.1111/phn.13028
- McLaughlin L, Khemthong U. The prevalence of type II workplace violence in US nurses 2000 to 2022: A meta-analysis. Western Journal of Nursing Research. 2024;46(3):248-255. doi:10.1177/01939459231222449
- Wallace D, Wang X. Does in-prison physical and mental health impact recidivism?. SSM-Population Health. 2020:11. doi:10.1016/j.ssmph.2020.100569
- Kendig N, Butkus R, Mathew S. Health care during incarceration: A policy position paper from the American College of Physicians. Annals of Internal Medicine. 2022;175(12):1742-1745. doi:10.7326/M22-2370
- Mechling B, Arms T. Losing to gain: The effects of a healthy lifestyle intervention on the physical and psychosocial well-being of clients in a community-based mental health setting. Community Mental Health Journal. 2019;55(4):608-614. doi:10.1007/s10597-019-00371-2
- Keller E, Boch S, Hittle B. Unsafe and unsettling. Journal of Forensic Nursing. 2022;18(4):229-236. doi:10.1097/JFN.0000000000000368
- Roberts D. Discover the benefits of correctional nursing. TKHealth. care. 2024. https://tkhealth.care/2024/11/13/discover-the-benefits-of-correctional-nursing/
- Johnson A, Reising V, Cruz C. Implementation of nursing services in community corrections: A community-academic partnership. Public Health Nursing. 2023;40(4):511-516. doi:10.1111/phn.13195
- Kucirka B, Ramirez J. Challenges of treating mental health issues in correctional settings. J Psychosoc Nurs Ment Health Serv. 2019;57(7):7-11. doi:10.3928/02793695-20190612-02
- Pelletier L, Vincent C, Woods L. Effectiveness of a psychiatric–mental health nurse residency program on retention. JAPNA. 2018;25(1):66-75. doi:10.1177/1078390318807968
- Hooper M, Virdun C, Phillips J. Capacity-building strategies that support correctional and justice health professionals to provide best-evidenced based healthcare for people in prison: A systematic review. IJEqH. 2025;24(1):115. doi:10.1186/s12939-025-02462-x
- Jones-Vanderleest J, Roosma-Goldstein S. Promoting interest in future correctional health care employment through a jail-based rotation for resident physicians. Journal of Correctional Health Care. 2025;31(2):77-81. doi:10.1089/jchc.24.08.0061
 This work is licensed under a
This work is licensed under a 