1.Introduction
1.1Problem description
Hospital waste presents both financial and environmental challenges. About 70% of hospital waste comes from the operating room and of that, anesthesia related supplies account for 25%.[1] This percentage is only expected to rise as reliance on single-use anesthesia items has grown significantly over the previous two decades, with the U.S. disposable medical device market reaching $66.9 billion in 2019 and growing annually at 16.7%.[2] Furthermore, the cost of single-use devices is likely underestimated, as full lifecycle cost of products which starts with raw material extraction and ends with waste processing, are often unclear.[3]
In addition to ballooning cost, current evidence shows that single use items have detrimental environmental effects, contributing directly to pollution and greenhouse gas emissions. In 2015, the World Health Organization attributed approximately 9 million deaths to pollution.[1, 3] Single use items typically require repeated manufacturing, packaging, and disposal, which increases greenhouse gas emissions and waste relative to reusable options. Indicative of these processes, supply chains account for an estimated 60%-80% of the overall healthcare sector’s greenhouse gas emissions.[4] In addition, most single-use supplies, and their packaging, are plastic. By 2050, the volume of plastic in the oceans is projected to outweigh fish, and micro and nanoplastics have been detected in rainfall, drinking water, human blood, and placental tissue.[4] Overall, these negative impacts highlight the need for interventions aimed at promoting environmentally sustainable and cost informed anesthesia practice that is not only safe for patients, but also beneficial for the world.
1.2Available knowledge
Despite a growing body of literature on anesthesia-related supply waste and its environmental impact, significant knowledge gaps exist.[1, 3, 5] Many anesthesia providers lack the knowledge to implement waste reduction strategies, and poor cost awareness contributes to excessive waste and increased expenses.[1, 6, 7] Systematic reviews reinforce the need for change, identifying institutional norms and limited provider education as barriers to sustainability thus emphasizing the importance of provider awareness in minimizing waste.[3, 5] Evidence further shows that anesthesia providers frequently underestimate costs, reinforcing the need for targeted educational interventions.[6]
International consensus also supports this, with the World Federation of Societies of Anesthesiologists calling for integration of sustainability into anesthesia practice.[8] One practical approach recommended by the Anesthesia Patient Safety Foundation (APSF), is utilization of a waste hierarchy tool (see Figure 1), which advises the order of actions to manage waste, from most to least environmentally preferred.[2] While “rethinking”, such as transitioning to reusable products, may not be feasible or timely at a large academic medical center due to logistical and operational challenges, focusing on waste reduction emerges as a particularly attractive and achievable option. Finally, multiple intervention studies demonstrate that targeted educational programs reduce waste across multiple aspects of anesthesia practice, producing measurable cost savings and environmental benefits, and highlighting education as an effective strategy for promoting sustainability in anesthesia care.[1, 5, 9,10,11]
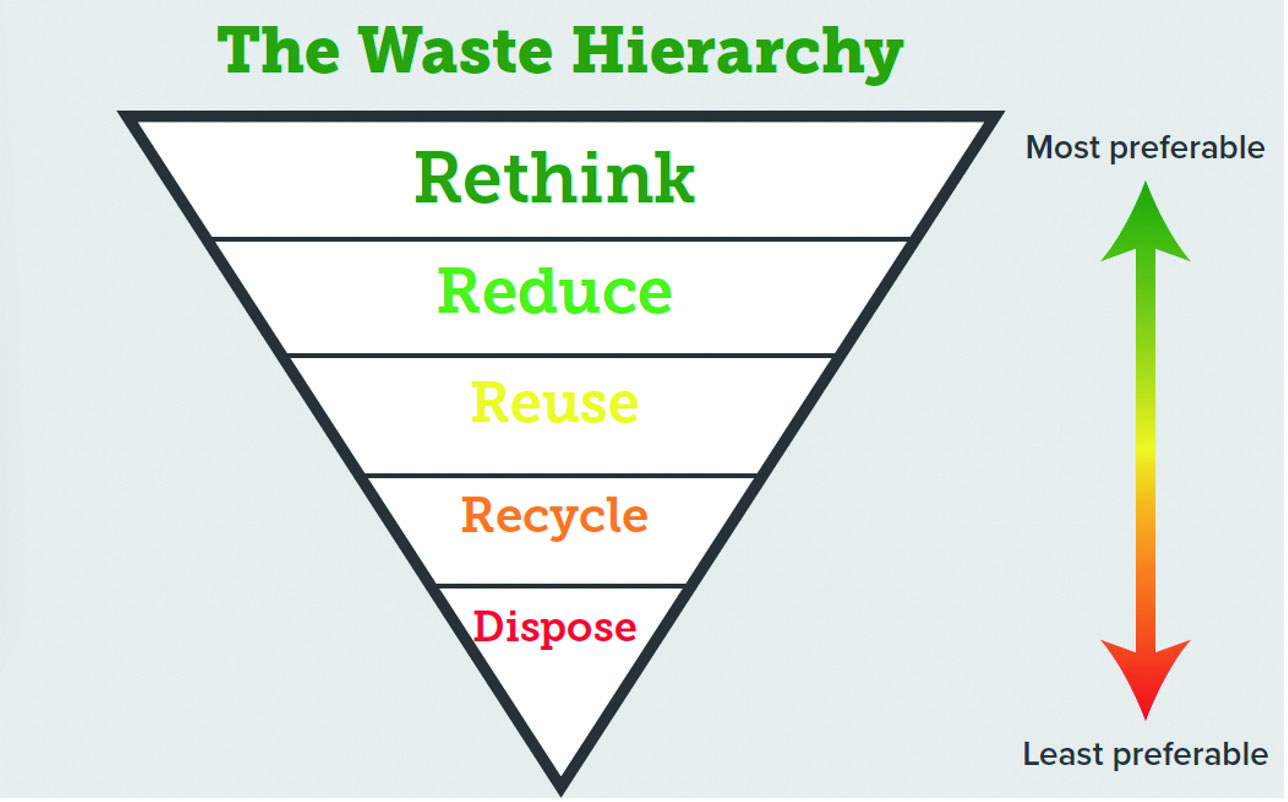
Figure 1.
APSF waste hierarchy tool
1.3Project purpose
This quality improvement (QI) project aims to reduce waste from single-use anesthesia supplies at a large academic medical center. The goal is to decrease financial losses from anesthesia supply waste over 10 days through an educational intervention for anesthesia staff. The intervention presents baseline waste data, educates providers on financial and environmental impacts, presents the cost of commonly used anesthesia supplies and introduces setup practice recommendations to reduce unnecessary supply use. Expected outcomes include a reduction in single-use supply waste and increased cost savings. By integrating evidence-based education and waste reduction strategies, this initiative seeks to improve sustainability and single use supply utilization.
1.4QI Model
The Institute for Healthcare Improvement (IHI)’s Model for improvement serves as the guiding framework for this project. It consists of three essential questions to define objectives, identify success measures, and determine effective interventions, using Plan-Do-Study-Act (PDSA) cycles to test and refine change.[12] This framework was chosen for its proven effectiveness in quality improvement initiatives. Its emphasis on small, incremental changes will enhance sustainability and its structured approach ensures improvements can be replicated in other hospital systems. By systematically evaluating changes and refining implementation strategies, the Model for Improvement provides a framework for achieving long-term impact.
2.Methods
2.1Context and intervention
This quality improvement project was conducted at a large academic medical center’s main campus operating rooms (ORs). Per The Joint Commission infection control guidelines, single use items like endotracheal tubes (ETTs) and laryngoscope blades are considered contaminated once their packaging has been opened and must be discarded, even if unused, to ensure hospital compliance.[13, 14] It was common practice for anesthesia providers to set up for cases before having a finalized anesthetic plan and to open various backup airways which can lead to an increased amount of opened but unused anesthesia supplies that must be wasted. The disposal of these opened but unused single use supplies represents a “double” waste, as these items are neither utilized in patient care nor repurposed, resulting in 100% financial and environmental loss. These materials, having been manufactured, sterilized, and transported, consume resources only to be discarded as mandated by The Joint Commission infection control guidelines, without ever serving their intended purpose.
Preintervention data collection served as baseline and was conducted over a 10-day period (Monday through Friday) in October 2024. This two-week period of representative sampling provides data reasonably representative of the total cases performed in one month when comparing case type, supplies utilized, and anesthesia providers. Weekend cases were excluded as the case volume and type can vary widely. Anesthesia technicians were instructed via email and shift huddles to leave opened, unused supplies out for collection rather than discarding them during room turnovers. The project team, with support from multiple Certified Registered Nurse Anesthetist (CRNA) volunteers, collected supplies from 27 ORs after the final case of each day. Off-site locations and cardiac ORs were excluded as their case volume can vary widely. These items were photographed, counted and total cost calculated utilizing an Excel collection tool.
An educational PowerPoint presentation was developed and delivered on three separate occasions in January 2025: once during department Grand Rounds and twice following didactic classes. This format ensured inclusion of the target population within the anesthesia department that includes approximately 104 CRNAs, 88 Student Registered Nurse Anesthetists (SRNAs), 70 attending anesthesiologists, and 28 anesthesia residents. The same slide deck was used for all three sessions, and the 30-minute presentation was intentionally structured to progress from global context to institution specific data and then to actionable practice changes. First, it presented an overview of the global financial and environmental impact of anesthesia supply waste and an explanation of life cycle costing (LCC) and life cycle assessment (LCA) using anesthesia specific examples to demonstrate how supplies that appear inexpensive at purchase contribute to higher long term financial and environmental costs when manufacturing, transport, and disposal are considered. Second, a discussion was held regarding the implications of the Joint Commission infection control guidelines and how opened, unused supplies must be discarded after each case to remain compliant. This portion of the education clarified that the intervention targeted changes in supply preparation behavior rather than deviations from infection prevention standards. Third, photos of collected opened, unused supplies (see Figure 2) and baseline collection data including both count and cost data in the form of pie charts and bar graphs were shared and thoroughly analyzed. This data was derived from the 10-day waste audit across the 27 operating rooms and included total cost, projected annualized cost, and individual item contribution to opened, unused waste to facilitate discussion of current preparation practices. Fourth, a pricelist of commonly used anesthesia supplies acquired from the institution purchasing department was shared to promote cost awareness and reinforce the financial impact of routine preparation behaviors.

Figure 2.
Baseline supply waste
Finally, sustainable practice recommendations based on the American Society of Anesthesiologists “Greening the Operating Room” document were shared and asked to be followed. Recommendations included: (1) Keep laryngoscope blades and ETTs in their unopened packaging until the anesthetic plan has been finalized, (2) Do not prepare ETTs or laryngoscope blades for the next patient until the current case has finished, (3) A backup ETT and laryngoscope blade should remain unopened.[4] Postintervention data collection was conducted identically to preintervention over a 10-day period in January 2025, from the same 27 ORs. Weekly follow-up emails and posted flyers posted in high traffic areas such as breakrooms and department common areas were used to encourage adherence to the new practice guidelines.
2.2Study of the intervention
A quantitative count tool was developed in Microsoft Excel to measure volume of single use anesthesia supply waste and associated cost. To ensure accuracy, a master price list was obtained from the hospital’s purchasing department. Each item was matched to its price via stock tag before being transcribed into the tool. Built-in formulas automatically calculated item costs, which were totaled for each 10-day period and compared between preintervention and postintervention. Descriptive statistics were used to analyze data between both periods. Visual data representations were created using Power BI and Excel, including a pie and bar chart illustrating cost savings by item, and a clustered bar chart comparing total waste volume and cost across the two periods.
2.3Ethical considerations
Ethical considerations were addressed through formal review and non-human subjects exception approval by the organization’s Institutional Review Board in December 2025. All data was collected in aggregate across the institution’s anesthesia department, with no identifiers linking data to individual providers. This approach ensured confidentiality and minimized the risk of bias or harm to participants. As the intervention focused on department-wide education and systems-level waste reduction, there were no anticipated conflicts of interest or ethical concerns related to individual performance evaluation or provider behavior tracking.
3.Results
Across the 10-day data collection periods, 24 distinct types of single use items were gathered. Direct laryngoscopy (DL) blades, ETTs, oral airways, stylets, oxygen tubing, syringes, and more, were collected. All categories showed a reduction in waste volume, with most also demonstrating cost savings (see Figure 3). The highest waste costs were associated with McGrath blades, DL blades, cuffed ETTs, flexible stylets and double lumen ETTs. High volume, lower cost items such as syringes, 4x4 gauze packs, and temperature probes also contributed to total waste.
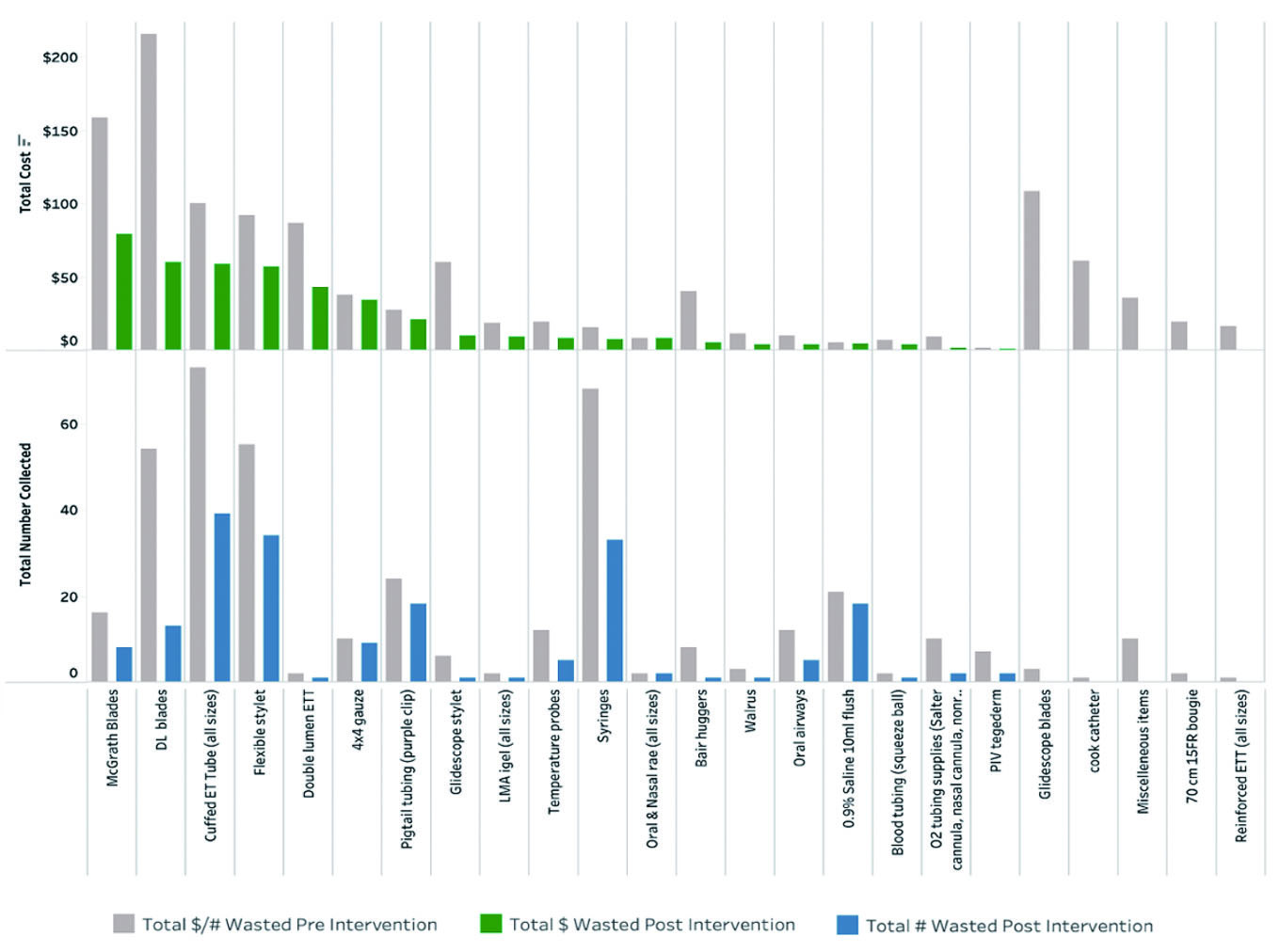
Figure 3.
Cost and number of wasted supplies pre and post intervention
During the post-intervention period, a total of 194 items were collected, down from 404 items pre-intervention, representing a 48% reduction in waste volume. The total monetary loss of wasted supplies decreased from $1,163.10 to $414.55, yielding a savings of $748.55 and a 64.4% increase in cost savings. This translated to a projected average total yearly loss of $29,077.50 pre-intervention, reduced to $10,363.75 post-intervention, resulting in estimated annual department savings of $18,713.75.
The delivery of the educational intervention remained consistent as the same PowerPoint presentation was provided on three occasions: once during department Grand Rounds and twice following didactic classes. No modifications were made to the educational content, format, or delivery approach. The only procedural difference between data collection periods was the personnel involved in supply collection. In the pre-intervention phase, CRNA volunteers participated in gathering supplies, while in the post-intervention phase, this responsibility was carried out solely by the DNP project team to enhance consistency during data collection.
No adverse patient care events, workflow delays, or supply shortages were reported as a consequence of the intervention. Separately, while anesthesia technician compliance with waste collection instructions was generally consistent, it is possible that some supplies were inadvertently discarded rather than saved for collection. Variability in staff scheduling limited attendance at the grand rounds educational session, however, this limitation was addressed through the dissemination of follow-up emails and posted flyers reinforcing the recommended practice changes. No missing data were reported, as all opened, unused supplies were systematically collected and recorded using the same structured audit tool, with pricing data from the established master price list applied consistently across both collection periods to ensure result comparability.
4.Discussion
4.1Summary
The volume of healthcare waste is unsustainable, both financially and environmentally, and this project highlights a practical solution to mitigate its impact. Project results demonstrated that a targeted, education-based intervention promoting cost awareness and providing sustainable practice recommendations significantly reduced unnecessary anesthesia supply waste while improving cost efficiency. Over a 10-day period, this intervention achieved a 48% decrease in overall waste volume and a 64% increase in cost savings, equating to a projected, estimated annual savings of $18,713.75. This demonstrates that an education-based intervention is a low-cost strategy that yields high financial savings and reduces anesthesia providers’ environmental impact. Despite being brief, the results support the integration of sustainability-focused education into anesthesia practice.
4.2Interpretation
The association between the educational intervention and reduced waste was direct and significant, as the introduction of evidence-based practice recommendations combined with education on the financial and environmental impact of anesthesia supply waste successfully influenced provider behavior. As anesthesia providers often lack visibility into supply prices, presenting baseline waste data alongside a supply pricing list reframed waste as a concrete financial loss rather than an abstract concept. Similarly, because the environmental impact of waste can also feel removed from daily clinical decisions, showing real time photographs of actual department supply waste from the hospital’s own cases, generated by the same anesthesia providers who received the education, made the issue tangible and linked daily practice to measurable cost and environmental outcomes. These results align with findings from prior studies that similarly reported provider education reduce waste and improve cost efficiency.[1, 5, 10, 11] The success of this intervention reinforces the role of anesthesia departments as change agents in broader hospital sustainability efforts.
From a cost perspective, the project demonstrated a clear return on investment. It required no upfront financial cost while opportunity costs included the labor involved in data collection and presentation preparation. These were minimized by involving CRNA volunteers during the pre-intervention phase and using existing department structures like Grand Rounds for education. Given these advantages, this project offers a replicable solution as healthcare institutions increasingly seek strategies that merge environmental responsibility with value-based care. Its strengths include simplicity, low cost, and ease of implementation using existing departmental infrastructure.
4.3Limitations
Limitations include the study’s short 10-day timeframe, which offers only a brief view of waste reduction outcomes. Additionally, some variation in the data may be attributed to contextual factors, such as instances where opened supplies were inadvertently discarded by anesthesia techs rather than saved for data collection, potentially leading to underreporting. The project was also limited by design to 27 ORs and did not include cardiac or off-site locations, which may have impacted the generalizability of the results. Lastly, the inability to deliver education to all anesthesia providers may have limited the full reach and effectiveness of the intervention.
5.Conclusions
The findings demonstrate that simple, education-based interventions can significantly reduce unnecessary single use supply waste and provide department cost savings. To sustain the impact of this work, next steps may include establishing regular waste collection audits for long-term follow-up and considering the formation of an anesthesia department sustainability committee. This project reinforces that addressing the environmental and financial impact of healthcare waste is not only necessary but that it is achievable through targeted, evidence-based education and daily practice change.
Authors contributions
All authors were equally responsible for study design, data collection, manuscript creation and revising. All authors read and approved the final manuscript.
Funding
Not applicable.
Conflicts of Interest Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
Not applicable.
References
- Denny N, Guyer J, Schroeder D. Operating room waste reduction. AANA J. 2019;87(6):477-482.
- Herr M, Segura L. Sustainable anesthesia: limiting waste, maximizing resiliency. APSF Newsl. 2023;38(3):96-99.
- Reynier T, Berahou M, Albaladejo P. Moving towards green anaesthesia: are patient safety and environmentally friendly practices compatible? A focus on single-use devices. Anaesth Crit Care Pain Med. 2021;40(4):100907. doi:10.1016/j.accpm.2021.100907
- American Society of Anesthesiologists. Greening the operating room and perioperative arena: environmental sustainability in anesthesia practice. Schaumburg (IL): American Society of Anesthesiologists. 2024.
- McGain F, Muret J, Lawson C. Environmental sustainability in anaesthesia and critical care. Br J Anaesth. 2020;125(5):680-692. doi:10.1016/j.bja.2020.06.055
- Qin C, Merkel K, Yesantharao L. Poor cost awareness among anesthesia providers for medications, supplies, and blood products. Jt Comm J Qual Patient Saf. 2020;46(9):524-530. doi:10.1016/j.jcjq.2020.06.007
- Gasciauskaite G, Lunkiewicz J, Spahn D. Environmental sustainability from anesthesia providers’ perspective: a qualitative study. BMC Anesthesiol. 2023;23(1):377. doi:10.1186/s12871-023-02344-1
- White S, Shelton C, Gelb A. World Federation of Societies of Anaesthesiologists Global Working Group on Environmental Sustainability in Anaesthesia. Principles of environmentally sustainable anaesthesia: a global consensus statement. Anaesthesia. 2022;77(2):201-212. doi:10.1111/anae.15598
- Sullivan G, Petit H, Reiter A. Environmental impact and cost savings of operating room quality improvement initiatives: a scoping review. J Am Coll Surg. 2023;236(2):411-423. doi:10.1097/XCS.0000000000000478
- Patel S, Smith-Steinert R. Greening the operating room, one procedure at a time. J Clim Change Health. 2021;2:100014. doi:10.1016/j.joclim.2021.100014
- Parilli-Johnson C, Pitman J, Barbee K. Implementation of a Power Down Initiative in 34 operating rooms. AANA J. 2024;92(4):257-268.
- Institute for Healthcare Improvement. How to improve: model for improvement. 2025 Oct 21. https://www.ihi.org/resources/how-improve-model-improvement
- The Joint Commission. Endotracheal tubes – clean, disinfect and store. 2013. https://pdfcoffee.com/standards-interpretation-joint-commission-pdf-free.html
- The Joint Commission. Laryngoscopes–blades and handles: how to clean, disinfect and store these devices. 2013. https://pdfcoffee.com/standards-interpretation-joint-commission-pdf-free.html
 This work is licensed under a
This work is licensed under a 