1.Background & purpose
Chest feeding (CF) is widely recognized as the optimal method of infant feeding, with numerous benefits for both parent and infant.[1] The terms CF and chest pumping (CP) are used to reflect inclusive language for lactation practices. They refer specifically to the mechanical or manual expression of human milk, aligning with inclusive language practices in perinatal and lactation care.[1, 2] The American Academy of Pediatrics and the World Health Organization recommend exclusive CF for the first six months of life, and support continued CF for two years or beyond.[1, 3] Human milk contains a dynamic and complex composition of antimicrobial, anti-inflammatory, and immunoregulatory components, all of which contribute to the healthy development of an infant’s immune system.[1] In terms of infant well-being, CF is associated with lower risk of sudden infant death; urinary tract, respiratory, and inner ear infections; and childhood obesity.[1, 4,5,6,7] CF also supports long-term parental benefits, including a reduced risk of type two diabetes mellitus, hypertension, and reproductive cancers.[1, 7] When infants are able to suckle, the release of oxytocin and prolactin not only promotes milk ejection and production, but assists in uterine involution and reduces risk of post-partum hemorrhage—important considerations in the critical care settings.[8,9,10] Despite these well-established benefits, postpartum patients admitted to intensive care units (ICUs) often face substantial barriers to initiating and maintaining lactation.[9,11,12]
Establishing lactation in a critically ill postpartum population requires timely assessment, appropriate interventions, and consistent support. However, one commonly encountered challenge is that many ICU nurses report feeling under-trained in managing CF-related care.[12] Another complicating factor in supporting lactation within the ICU setting is that nurses are tasked with performing frequent and time-sensitive interventions due to patient complexity. This leaves limited opportunity to dedicate the 15-60 minutes required for lactation support every two to three hours.[9] Time and workload constraints are well-recognized barriers in critical care environments, where competing priorities often limit nurses’ ability to provide sustained lactation-related care.[9, 12, 13] While long-term sustainability of support may benefit from administrative engagement, this educational intervention was intentionally designed to be brief and integrated into clinical workflow within existing staffing structures. Future initiatives may further strengthen implementation through formal leadership support.[14, 15] Additionally, the urgency of critical illness often shifts clinical priorities to physiological stabilization, resulting in omission of lactation during vital windows of milk production.[9] When lactation support is delayed, complications such as engorgement, mastitis, or breast abscesses can occur, resulting in pain, infection, and in some cases, the need for surgical resection.[16]
Engorgement typically arises three to seven days postpartum and results from infrequent or ineffective milk removal. It is a major contributor to lactation-related discomfort and early lactation cessation.[16] ICU nurses should be knowledgeable in order to initiate milk supply, using expression techniques to prevent engorgement, and facilitating CF once the patient’s condition permits.[9] Mastitis is a bacterial chest infection that affects up to three percent of CF patients. It is often preceded by unresolved engorgement and exacerbated by stress and fatigue – conditions commonly seen in ICU patients.[16] Without proper support, some patients are unable to establish a milk supply at all, undermining optimal parental and neonatal health outcomes.[9, 12] Given the immunologic and hormonal processes involved in lactation, early intervention is essential. Yet, current practices in critical care lack emphasis on CF support.[7]
Institutional CF policies can have a significant influence on CF success rates, yet such policies are often underdeveloped or are inconsistently applied in critical care settings.[9, 17] It is well documented that implementing hands-on strategies and improving nursing knowledge can improve CF, in turn reducing risks and improving health benefits for parent and child.[7, 9, 18] The purpose of this quality improvement project was to evaluate the impact of a structured, evidence-based educational intervention on ICU nurses’ knowledge and adherence to best practices for CF in the care of critically ill postpartum patients.
Framework
The Knowledge-to-Action (KTA) Framework was chosen to guide this project because of its practical, cyclical structure that bridges the gap between evidence-based knowledge and real-world application.[19] The KTA Framework is particularly well-suited for an ICU nursing initiative as it emphasizes both generation and active use of knowledge through collaboration and implementation.
During the knowledge inquiry phase, a critical educational gap was identified related to CF in the ICU. This is supported by literature outlining unique challenges faced by these critically ill patients. For the knowledge synthesis stage, a review of current guidelines and best practices was compiled into a cohesive protocol. This protocol served as the foundation for both the pre- and post-evaluation tool.
The action cycle of the KTA Framework was also integrated in this project. The intervention was tailored to the designated ICU through direct input from stakeholders, including ICU nurse educators, the clinical care lead, and lactation consultants. Barriers to knowledge use, such as staff time constraints, little previous training, and limited comfort with CF care, were identified early on and addressed through our design of a short, targeted teaching session implemented at the bedside. Finally, mechanisms for sustainability were discussed with stakeholders, including the potential integration of this teaching into new hire orientation. Short videos of chest pump set up, initiation, and cleaning are available in the protocol for easy referencing. By aligning each phase of the project with the steps of the KTA Framework, this initiative not only addressed an immediate educational need, but laid groundwork for future training and practice.
2.Methods & analysis
This project used a pre-post intervention quantitative design and began in January 2025. A series of bedside education sessions occurred over a two-week period, each approximately 15 minutes in length. Participants were ICU registered nurses, recruited based on availability and were provided with information about the project objectives, voluntary nature, and confidentiality safeguards. Pre-education intervention data was collected through an evaluation tool, created based on the facilities ICU pumping protocol, to assess participants’ initial ability to complete the pumping process. The educational intervention was developed collaboratively with ICU nurse educators and lactation consultants and was grounded in current institutional protocols and evidence-based lactation guidelines. Education was delivered at the bedside in brief sessions using a standardized script to ensure consistency. Instruction included hands-on demonstration of setup, initiation, hand expression techniques, and equipment cleaning using a mannequin and visual aids. This approach was intentionally designed for ICU nurses without prior labour and delivery experience and emphasized practical skill acquisition within routine clinical workflows. Following the intervention, post-assessments were conducted and evaluated using the same evaluation tool. Data extraction was conducted by sorting information into a tally sheet using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA, 2024) and analyzed using SPSS software (IBM Corp., Armonk, NY, USA 2021). Pre- and post-intervention scores were compared by
Ethical considerations
Research ethics approval was granted by the University of Ottawa Research Ethics Board. This quality improvement project was conducted in a tertiary-care adult intensive care unit within a large academic teaching hospital. To minimize any perceived coercion, participation was voluntary, recruitment was conducted independent of unit leadership, and nurses were informed that participation or non-participation would have no impact on employment status, performance evaluation, or scheduling. Participants were provided the opportunity to decline or withdraw at any time without consequence. Prior to data collection, the project objectives were clearly explained and verbal informed consent was obtained from each participant, including an opportunity to ask questions or decline involvement. Responses were recorded confidentially without any identifying information. Data was arranged in aggregate format, only allowing overall trends to be traceable through charts and graphs. All data was stored digitally, password protected and shared exclusively with project stakeholders upon request. This approach protected participant privacy and upheld ethical standards for educational research.
3.Results
A total of 60 ICU registered nurses were recruited. The mean age of participants was 37.1 years (SD 10.53 years; range 23-60). The group had a mean of 11.1 years (SD 8.69 years) of clinical experience, reflecting a diverse mix of early-career and seasoned practitioners. Of these participants, 50 (83%) identified as female and 10 (17%) as male. None of participants had previous experience working in a labour and delivery unit. All participants who were approached regarding this project were recruited and there was no attrition.
Following completion of the educational session, adherence to all steps of the chest pumping process improved significantly (
| Initiation | < .001 | |||||
| Hand washing | 17 (28.3) | 43 (71.7) | 56 (93.3) | 4 (6.7) | ||
| Phalange sizing | 8 (13.3) | 52 (86.7) | 59 (98.3) | 1 (1.7) | ||
| Pump set-up | 8 (13.3) | 52 (86.7) | 57 (95.0) | 3 (5.0) | ||
| Placing the shield | 19 (31.7) | 41 (68.3) | 60 (100.0) | 0 (0.0) | ||
| Power on and press the “let down” | 2 (3.3) | 58 (96.7) | 57 (95.0) | 3 (5.0) | ||
| Cleaning | ||||||
| Wash pump parts | 30 (50.0) | 30 (50.0) | 60 (100.0) | 0 (0.0) | < .001 | |
| Place on dry towel/sterilize | 5 (8.3) | 55 (91.7) | 59 (98.3) | 1 (1.7) | ||
| Hand compression | < .001 | |||||
| Wash hands | 9 (15.0) | 51 (85.0) | 56 (93.3) | 4 (6.7) | ||
| Massage breasts | 3 (5.0) | 57 (95.0) | 50 (83.3) | 10 (16.7) | ||
| Place fingers one inch from nipple, in shape of “C” | 4 (6.7) | 56 (93.3) | 59 (98.3) | 1 (1.7) | ||
| Nipple pulsation | 12 (20.0) | 48 (80.0) | 60 (100.0) | 0 (0.0) | ||
| Drop gathering | 4 (6.7) | 56 (93.3) | 60 (100.0) | 0 (0.0) | ||
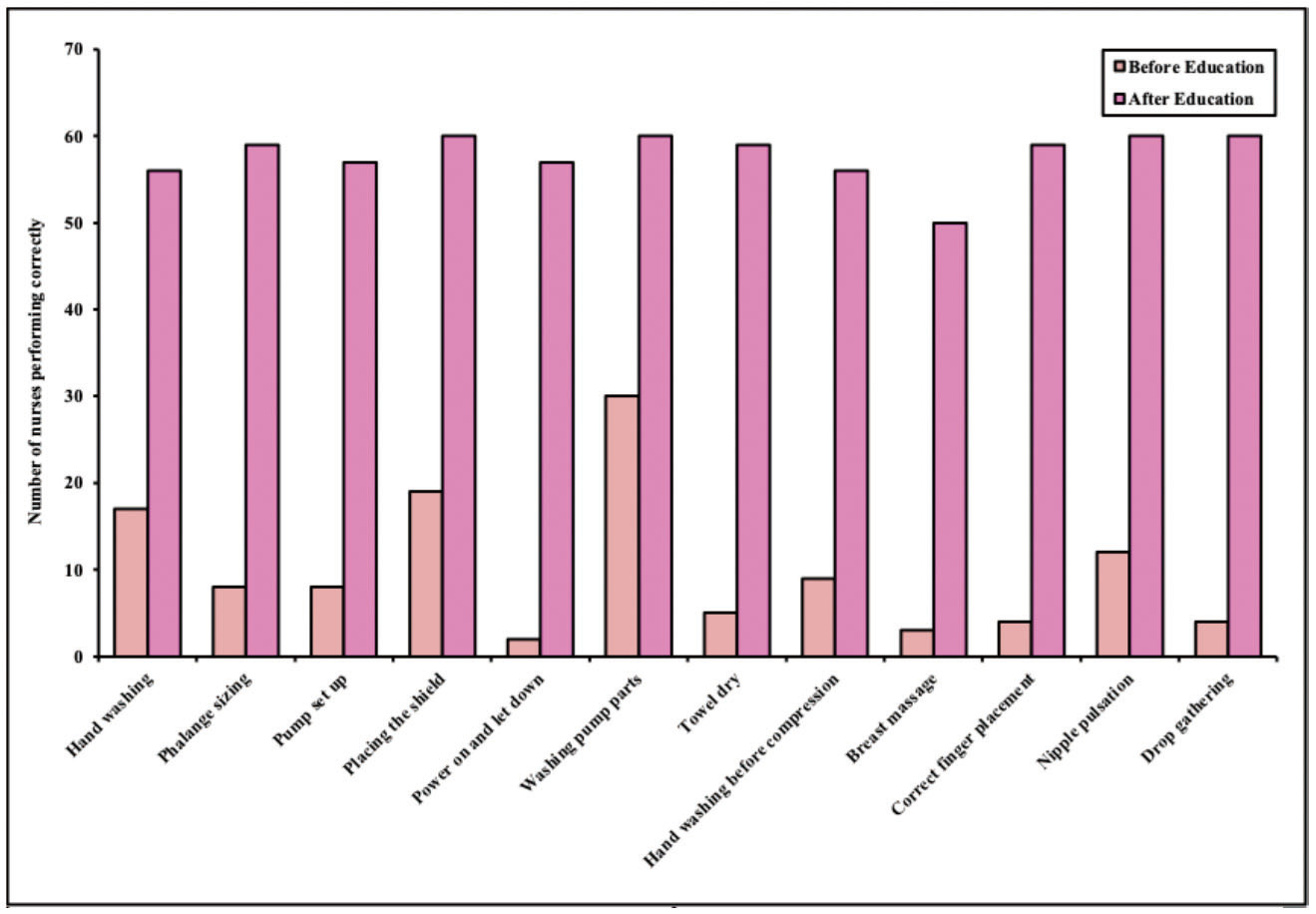
Figure 1.
Nurses’ success before and after educational session intervention by step
4.Discussion
ICU nurses endorse feelings of discomfort, absence of confidence, and lack in competence in meeting the needs of postpartum patients, particularly with CF.[9, 12, 13, 20, 21] Although there is extensive research focusing on the benefits and maintenance of healthy lactation among postpartum patients, there is a paucity of guidance specific to the critical care setting.[13, 22]
4.1Quality improvement uptake
In order to improve patient outcomes and safe provision of care, nurses generate interventions to address arising problems; this is critical for improving and advancing nursing practice.[15, 23] There are many factors that contribute to the update of quality improvement initiatives. Ground-up, practitioner-led work is often an adequate response to a raised concern. Those actively engaging with an issue often provide the greatest insight, and are uniquely positioned to identify areas of improvement, and implement changes that are practical—particularly when supported with the time and skills to do so.[14] Improvements to accountability practices, such as provision of increased training opportunities, are associated with greater quality improvement uptake.[24] Factors such as high turnover of leadership, lack of focus, and poor external relationships among various stakeholders are detrimental to quality improvement;[25, 26] these issues did not arise in the current study.
4.2Advanced practice nursing competencies
Advanced practice nurses (APNs) are key drivers in implementing and sustaining both practice and organizational change. According to Advanced Practice Nursing: A Pan-Canadian Framework (2019), APNs demonstrate competencies in clinical care, leadership, research, education, collaboration, and health systems.[27] APNs play a central role in initiating, implementing, and sustaining evidence-informed practice change within healthcare. They are uniquely equipped to bridge the gap between research and clinical care through exposure to research and completion of advanced competencies. Their advocacy skills allow them to influence policy and promote a culture of growth and improvement.[27]
4.3Limitations
While the intervention was effective, several limitations must be acknowledged. First, the project was conducted in a single ICU setting with a relatively small sample size which may limit generalizability of findings. Second, performance was assessed immediately after the educational sessions; therefore, long-term retention cannot be ascertained. Future efforts should involve reassessment of CF performance following the educational sessions to evaluate sustained learning over time. A valuable lesson learned throughout this project was the importance of creating opportunities for hands-on learning and immediate feedback, which appeared to enhance engagement and confidence. We also acknowledge that several sources are outdated. However, they remain highly relevant, as limited contemporary literature exists addressing lactation support and CF practices within adult critical care settings. While room for improvement exists, the consistency of statistical significance across all areas of this education underscores the value of targeted educational initiatives in enhancing evidence-based lactation support in critical care settings.
5.Conclusion
Through alignment with the KTA Framework, this initiative translated current best practices into actionable and sustainable bedside teaching tailored to the realities of critical care. The statistically significant improvements highlight the impact of focused interventions that are often overlooked. Sustaining this new CF initiative will require ongoing education, reinforcement of protocols, and continued prioritization of CF—and postpartum care as a whole—into the usual critical care paradigm. This initiative contributed meaningfully to patient- and family-centered care and reinforces the essential role of ICU nurses in supporting optimal lactation outcomes in postpartum patients with critical illness.
Authors contributions
All authors contributed to the study’s conception and writing. The project was completed by T.M.B, and the original manuscript was completed by T.M.B. The project was supervised by C.G., J.S., and B.V-W. D.B and A.W provided figure production. The manuscript was reviewed, edited, and approved by all authors.
Funding
This project does not have any funding sources to disclose.
Conflicts of interest disclosure
The authors declare that they have no competing interests to declare.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
We greatly appreciate the contributions of each nurse who participated in our educational intervention.
References
- Meek J, Noble L. Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics. 2022;150(1):e2022057988. doi:10.1542/peds.2022-057988
- American Academy of Pediatrics (AAP). Words Matter: AAP Guidance on Inclusive, Anti-biased Language. May. 2021. https://www.aap.org/en/about-the-aap/american-academy-of-pediatrics-equity-and-inclusion-efforts/words-matter-aap-guidance-on-inclusive-anti-biased-language/
- World Health Organization. Infant and young child feeding. 2023. https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
- Bowatte G, Tham R, Allen K. Breastfeeding and childhood acute otitis media: a systematic review and meta-analysis. Acta Paediatrica. 2015;104(467):85-95. doi:10.1111/apa.13151
- Chen A, Rogan W. Breastfeeding and the Risk of Postneonatal Death in the United States. Pediatrics. 2004;113(5):e435-e439. doi:10.1542/peds.113.5.e435
- Quigley M, Carson C, Sacker A. Exclusive breastfeeding duration and infant infection. Eur J Clin Nutr. 2016;70(12):1420-1427. doi:10.1038/ejcn.2016.135
- Stuebe A. The risks of not breastfeeding for mothers and infants. Rev Obstet Gynecol. 2009;2(4):222-231.
- Anderson G. The Mother and Her Newborn: Mutual Caregivers. JOGN Nursing. 1977;6(5):50-57. doi:10.1111/j.1552-6909.1977.tb02181.x
- Dauphinee J, Amato K, Kiehl E. Support of the Breast-Feeding Mother in Critical Care. AACN Clinical Issues: Advanced Practice in Acute and Critical Care. 1997;8(4):539-549. doi:10.1097/00044067-199711000-00004
- Lawrence R. The clinician’s role in teaching proper infant feeding techniques. The Journal of Pediatrics. 1995;126(6):S112-S117. doi:10.1016/S0022-3476(95)90250-3
- Kolbe K, Sheffield V, Castillo K. Lactation Practices in Critically Ill Patients. CHEST Critical Care. 2025;3(1):100123. doi:10.1016/j.chstcc.2024.100123
- Pollock W. Caring for pregnant and postnatal women in intensive care: What do we know?. Australian Critical Care. 2006;19(2):54-65. doi:10.1016/S1036-7314(06)80010-X
- Kynoch K, Paxton J, Chang A. ICU nurses’ experiences and perspectives of caring for obstetric patients in intensive care: a qualitative study. Journal of Clinical Nursing. 2011;20(11–12):1768-1775. doi:10.1111/j.1365-2702.2010.03517.x
- Allwood D, Fisher R, Warburton W. Creating space for quality improvement. BMJ. 2018:k1924. doi:10.1136/bmj.k1924
- Asurakkody T, Shin S. Innovative Behavior in Nursing Context: A Concept Analysis. Asian Nursing Research. 2018;12(4):237-244. doi:10.1016/j.anr.2018.11.003
- Mass S. Breast Pain: Engorgement, Nipple Pain and Mastitis. Clinical Obstetrics and Gynecology. 2004;47(3):676-682. doi:10.1097/01.grf.0000135652.49154.75
- Ellis D. The impact of agency policies and protocols on breastfeeding. NAACOGS Clin Issu Perinat Womens Health Nurs. 1992;3(4):553-559.
- Kramer M, Chalmers B, Hodnett E. Promotion of Breastfeeding Intervention Trial (PROBIT): A Randomized Trial in the Republic of Belarus. JAMA. 2001;285(4):413-20. doi:10.1001/jama.285.4.413
- Graham I, Logan J, Harrison M. Lost in knowledge translation: Time for a map?. Journal of Continuing Education in the Health Professions. 2006;26(1):13-24. doi:10.1002/chp.47
- Campbell P, Rudisill P. Psychosocial needs of the critically ill obstetric patient: the nurse’s role. Crit Care Nurs Q. 2006;29(1):77-80. doi:10.1097/00002727-200601000-00008
- Zisin Y, Clarke A, Kloester J. Exploring Australian intensive care unit nurses’ experiences, confidence, and knowledge in supporting breastfeeding women in the early postpartum period: A descriptive cross-sectional study. Australian Critical Care. 2026;39(1):101467. doi:10.1016/j.aucc.2025.101467
- Schack-Nielsen L, Michaelsen K. Breast feeding and future health: Current Opinion in Clinical Nutrition and Metabolic Care. 2006;9(3):289-296. doi:10.1097/01.mco.0000222114.84159.79
- Younas A. Uptake of Innovations in Nursing: The Necessity for Implementation Science. Creative Nursing. 2023;29(2):177-181. doi:10.1177/10784535231195426
- Bate P, Mendel P, Robert G. Organizing for Quality: The Improvement Journeys of Leading Hospitals in Europe and the United States. CRC Press. 2007. doi:10.1201/b20730
- Jones L, Pomeroy L, Robert G. How do hospital boards govern for quality improvement? A mixed methods study of 15 organisations in England. BMJ Qual Saf. 2017;26(12):978-986. doi:10.1136/bmjqs-2016-006433
- Vaughn V, Saint S, Krein S. Characteristics of healthcare organisations struggling to improve quality: results from a systematic review of qualitative studies. BMJ Qual Saf. 2019;28(1):74-84. doi:10.1136/bmjqs-2017-007573
- Canadian Nurses Association. Advanced Practice Nursing: A Pan-Canadian Framework. 2019. https://hl-prod-ca-oc-download.s3-ca-central-1.amazonaws.com/CNA/2f975e7e-4a40-45ca-863c-5ebf0a138d5e/UploadedImages/documents/nursing/Advanced_Practice_Nursing_framework_e.pdf
 This work is licensed under a
This work is licensed under a 