1.Background
Cognitive impairment is a prevalent and distressing concern among individuals receiving palliative care. In a retrospective cross-sectional analysis, Watt and colleagues (2021) observed that its prevalence, including delirium, ranged from 13.3% to 42.3% at the time of admission, increased to 26%-62% during the hospital stay, and surged to 58.8%–88% in the final days or hours of life.[1] Delirium stands out as the most common neuropsychiatric condition in this context, with up to 80% of patients with advanced cancer experiencing it at the end of life.[2] Despite its frequency, hypoactive delirium often goes unrecognized largely because its symptoms overlap with those of dementia and depression, complicating timely diagnosis.[1, 3] In the early stages of the cancer trajectory, delirium is often acute reversible conditions that can be treated by identifying the underlying causes, such as infection, dehydration, electrolyte imbalance, and medications.[4]
Early identification of delirium may be improved by the combination of clinical judgement and using of validated screening tools by health care providers and nursing staff. Frequently utilized screening tools comprise the Confusion Assessment Method (CAM), which uses an algorithm that requires positive results. While the CAM-ICU is an intensive care variant of the CAM tool.[1] The Nursing Delirium Scale (Nu-DESC) was validated to be used by nurses and caregivers. In addition, Memorial Delirium Assessment Scale (MDAS) was validated in different languages and used on in-patients’ oncology population.[1] Additional tools are not only designed for delirium but may also be utilized to assess cognitive function, such as the Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE).[1] Scales differ according to the cognitive domains they emphasize, the total duration required for completion, and additional variables.
Problem
In palliative care settings, the early identification of delirium in patients with advanced cancer is crucial not only for alleviating distressing symptoms in patients and families, but also for enabling timely interventions. The MMSE, first introduced in 1975 ,[5] has been employed in palliative care populations since 1999.[6] A review by Hjermstad, Loge, and Kaasa (2004) revealed that the MMSE was utilized in 13 out of 22 studies evaluating cognitive impairment in palliative care.[7] However, despite its widespread use, the MMSE has never been formally validated for use in palliative care populations.[2]
Multiple reviewers have raised concerns regarding the MMSE’s suitability in this setting, particularly for patients with advanced progressive cancer.[2, 8] In this population, the MMSE is often perceived as lengthy, burdensome, and impractical for routine use. To address these limitations, a shortened version comprising four of the original 20 MMSE items has been proposed as a more feasible alternative for detecting early cognitive decline in advanced cancer patients.[2] Supporting this concern, prior research has shown that 22% of patients were unable to complete the full MMSE, 12% omitted the final two items, and only 66% were able to complete the test in its entirety. These difficulties were especially pronounced in items requiring more complex tasks, such as following three-step commands, reading, writing, and drawing a pentagon, all of which are part of the original MMSE tool.[8, 9] This aligns closely with our own clinical experience using the MMSE in patients newly accepted under palliative care with advanced malignancies.
At the National Center for Cancer Care and Research (NCCCR) in Qatar, the MMSE has been in routine use by the palliative care team for the past 14 years to assess cognitive function at the time of patient acceptance. However, it has consistently proven to be challenging and impractical for patients, caregivers, and clinicians alike, failing to capture cognitive status adequately in this frail, vulnerable population. Given the advanced disease state, diminished performance status, and limited life expectancy of these patients, a brief, user-friendly, reliable tool is essential for appropriate cognitive evaluation.
The Assessment Test for Delirium and Cognitive Impairment (4AT) is a well-validated bedside screening tool specifically designed for rapid identification of delirium and cognitive impairment in clinical practice.[10, 11] In contrast to the MMSE, the 4AT is brief (requiring only 2–3 minutes to complete), simple to administer, and does not necessitate formal training. A recent systematic review and meta-analysis involving 17 studies and 3,702 patients confirmed its diagnostic robustness, demonstrating a pooled sensitivity and specificity of 88% each.[4] The tool has been shown to significantly improve detection rates of delirium when routinely implemented across healthcare settings.[12] Its straightforward design, comprising only four items, along with its availability in both Arabic and English, further enhances its suitability for use in our diverse patient population, including Arabic-speaking individuals. Importantly, the 4AT has also been validated in palliative care settings.[12]
This quality improvement project aims to enhance current clinical practice by evaluating the 4AT tool against the MMSE for the initial cognitive assessment of patients with advanced cancer upon acceptance into the palliative care program. The goal is to determine whether the 4AT can provide a more effective, practical, and compassionate approach to early detection of delirium and cognitive decline in this sensitive patient group.
2.Method
A quality improvement initiative was undertaken using the Plan-Do-Study-Act (PDSA) methodology to optimize the process of initial cognitive assessment for patients on their first day of acceptance into the palliative care program. As part of this initiative, 53 patients with advanced cancer were assessed using both the MMSE and the 4AT screening tools, with versions available in both Arabic and English. The assessments were performed on the day of admission to ensure early identification of cognitive impairment or delirium. After the implementation phase, a survey was given to palliative care doctors to gather their thoughts and experiences about how useful, easy to use, and effective the 4AT tool was compared to the MMSE.
2.1Design
The study was conducted at NCCCR in Qatar, among newly accepted palliative care patients, between July 2022 and February 2023. The team adopted the model for Improvement framework, which utilizes the PDSA methodology, to test and implement changes within the supportive and palliative care program. It was determined that a series of PDSA cycles would be conducted, with each cycle followed by an evaluation phase to assess outcomes and inform further refinement.
The staff provided feedback on the benefits and challenges of the implemented modifications. We aimed to identify the most practicable instrument for assessing patients’ cognitive states in the palliative care service, which we could then recommend for amendment in our policy, using numerous PDSA cycles. By emphasizing the significance of early identification and treatment of delirium in enhancing patient outcomes, staff were further motivated to participate in the proposed modifications. The baseline data demonstrated that the MMSE documentation was not promoting formal cognitive assessment during patient admission under the palliative care program. Medical colleagues concurred that the current procedures necessitated modification, and they expressed a willingness to evaluate the 4AT on our palliative care patient population and provide feedback on the usability of these tools among patients admitted under the palliative care program.
2.2Strategy
2.2.1PDSA 1
A brief survey was developed and tested to measure supportive and palliative care unit (SPCU) physicians’ perceptions of using the MMSE as an initial cognitive assessment tool in palliative care practice. We requested the eight SPCU physicians to complete the brief survey that included four questions on their experiences and perceptions of utilizing the MMSE. The physicians’ feedback helped to understand the deterrents of using MMSE. Baseline data was collected after using the brief survey. Accordingly, the 4AT was then introduced and requested by SPCU physicians to use it in addition to the policy-supported MMSE instrument (see Figure 1).
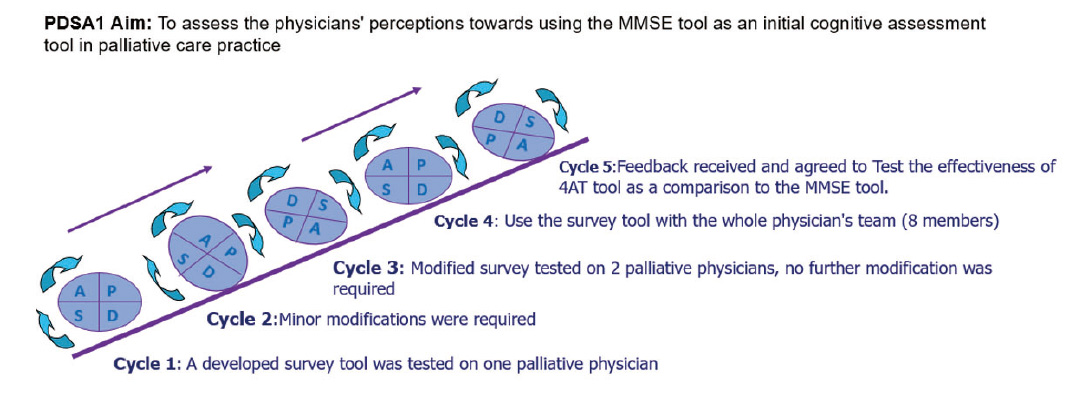
Figure 1.
Cycle 1 of the PDSA
2.2.2PDSA 2
Another cycle of change was conducted using the 4AT tool for the delirium and cognitive assessment of patients on the first day of their acceptance under the program by the SPCU physicians. A palliative care physician tested the 4AT tool on a single patient. The tool was then utilized alongside the MMSE tool for 20 patients (see Figure 2).
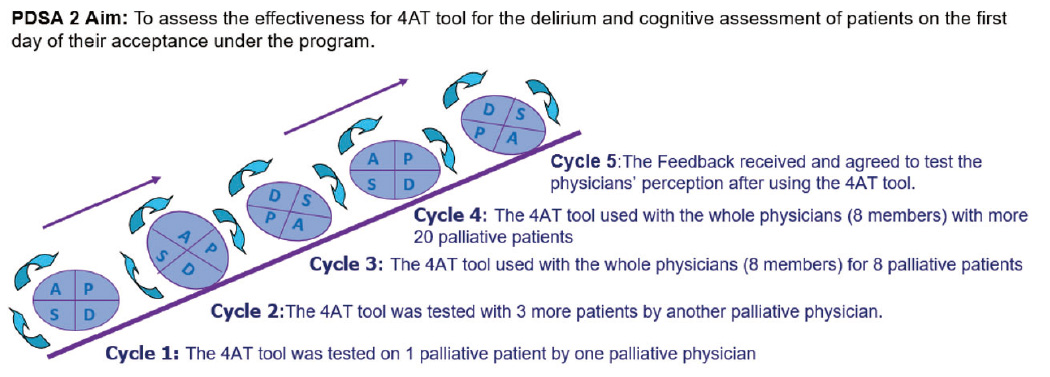
Figure 2.
Cycle 2 of the PDSA
2.2.3PDSA 3
After reviewing all the findings, our project team decided to use the same brief survey method for 4AT as a comparison to the MMSE tool with the same eight SPCU physicians. The survey was adapted, tested, and used with SPCU physicians to answer questions about their experience using the 4AT tool. To validate the findings, the physicians chose to administer the MMSE and the 4AT instrument to an additional 33 new patients (see Figure 3).
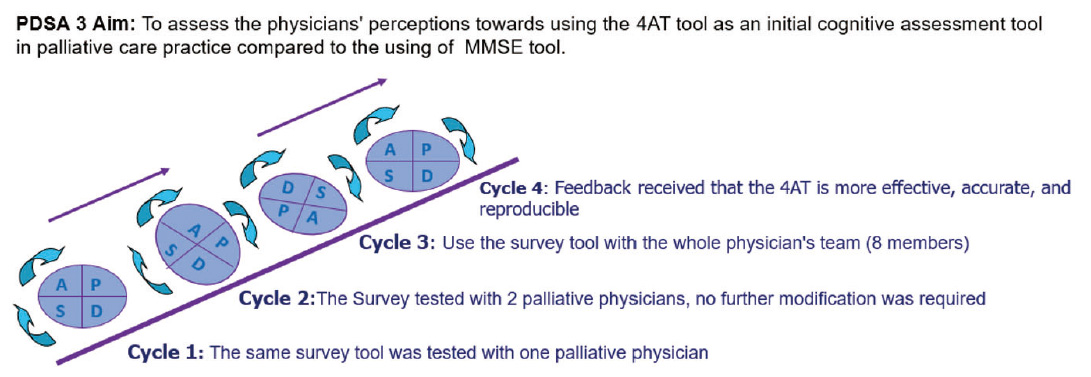
Figure 3.
Cycle 3 of the PDSA
3.Result
The study compared the data from the pre-implementation of the MMSE tool to that after the introduction of the 4AT from 2nd quarter of 2022 to 2nd quarter of 2023. A survey conducted among eight palliative care physicians revealed that 63% found the MMSE tool to be too lengthy, 87.5% (7 out of 8) believed it provided insufficient information, 63% (5 out of 8) thought it was challenging for patients to understand, and 75% found it difficult to complete. In contrast, 100% of the physicians found the 4AT tool to be simpler and easier to complete. They reported it as 75% effective in assessing cognitive status, indicated that 62.5% found it useful, and stated that 100% believed it was better accepted by palliative care patients compared to the MMSE. The results suggest that the 4AT tool is a more appropriate option for clinical practice in palliative care (see Figure 4).
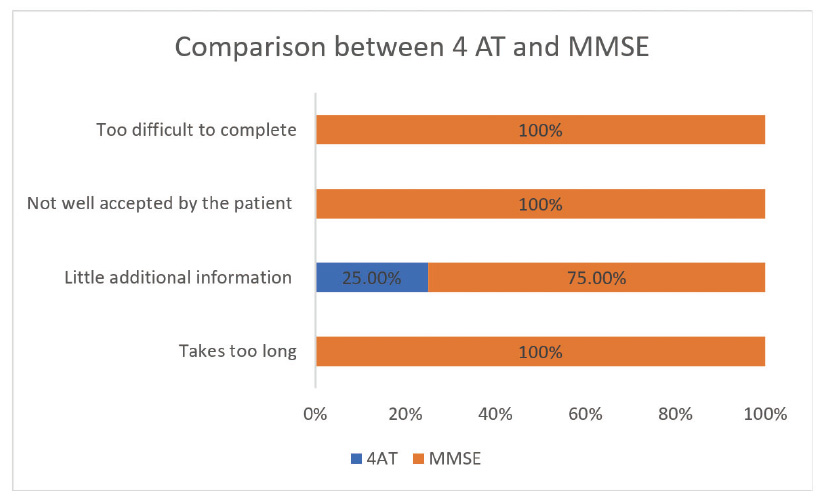
Figure 4.
Comparison between 4AT and MMSE tools
4.Discussion
The findings of this quality improvement project clearly demonstrate that the 4AT tool offers distinct advantages over the MMSE for the initial cognitive assessment of patients with advanced cancer upon admission to the palliative care program. The 4AT was consistently found to be shorter, easier to administer, more practical, and more user-friendly. Its brevity and simplicity enabled SPCU physicians to complete the assessment efficiently during initial evaluations, resulting in greater adherence to cognitive screening protocols.
To our knowledge, this is the first study conducted in the Middle East and Gulf region to directly compare the feasibility and utility of the 4AT and MMSE tools in assessing cognitive status among patients with advanced cancer receiving palliative care. Initial cognitive assessment is a critical component of comprehensive palliative evaluation. Early identification of cognitive changes, particularly delirium, is essential for ensuring high-quality care, facilitating communication among healthcare professionals, and supporting families and caregivers.[12] Routine cognitive screening during the first evaluation phase enables early detection and management of potentially reversible disorders such as delirium, ultimately contributing to better therapeutic results.[13]
Although the MMSE remains a widely recognized and validated tool for cognitive assessment, especially in general medical and geriatric populations, its application in advanced cancer patients within palliative care presents notable limitations. In this population, which is characterized by frailty, low performance status, and reduced attention span, the MMSE is often too time-consuming and less suitable for bedside screening. Some studies have proposed using abbreviated versions of the MMSE to improve its practicality.[2, 8] However, completion rates remain suboptimal, as many patients struggle with tasks that require reading, writing or drawing.[8, 9] Our clinical experience reflects these challenges, confirming the limitations of the MMSE in this context.
Since its development and validation in 2014, the 4AT tool has emerged as a reliable and efficient alternative for rapid screening of delirium and cognitive impairment. Baird and Spiller (2017) reported that the 4AT performed on par with the short CAM, while offering superior usability during hospice admissions. In their study, cognitive screening compliance increased from 0% to 76%, after integrating the 4AT or short CAM, into admission procedures.[14] Healthcare staff consistently described the 4AT as clear, brief, and easy to administer, even with minimal or no prior training.[15] The underutilization of cognitive assessments in some clinical settings has been attributed to the absence of accessible, efficient tools an issue that the 4AT effectively addresses.[13]
Among several internationally recognized cognitive screening instruments, the 4AT stands out because of its concise format, ease of application, lack of training requirements, and availability in multiple languages, including Arabic. These factors make it highly appropriate for use in our culturally diverse population. The role of the 4AT in facilitating early detection of cognitive impairment and delirium is increasingly supported by a robust and growing body of literature.[13, 16, 17, 18, 19, 20]
Based on the results of this project, it was recommended that the 4AT to be used in place of the MMSE tool and make necessary changes in the policy, aiming to improve the practice of the initial cognitive assessment of patients who have been completely transferred under the palliative care program. Building upon the success of this initiative, future efforts will aim to broaden the use of the 4AT beyond patients formally enrolled in the palliative care program, extending its application to oncology inpatients receiving palliative consultations. This expansion is anticipated to further enhance the timely identification and management of cognitive disturbances in a highly vulnerable patient population.
5.Conclusion
This quality improvement project underscores the 4AT tool as a highly effective, practical, and well-accepted instrument for the initial assessment of cognitive function and early detection of delirium in patients with advanced cancer upon their entry into the palliative care program. Its demonstrated efficacy, user-friendliness, and rapid administration make it exceptionally suited to the needs of this vulnerable population. Considering these findings, palliative care physicians at our center have strongly endorsed the 4AT as the preferred alternative to the MMSE for routine cognitive screening marking a significant advancement in the delivery of timely, compassionate, and evidence-based palliative care.
Authors contributions
Shaikhah Al-Keldi conceptualized and designed the project, developed the survey instrument, supervised data collection, conducted data analysis, drafted the initial manuscript, and critically reviewed the final manuscript. Dr. Ayman Allam contributed to drafting the initial manuscript, reviewing and testing the tools. Dr. Azar Saleem reviewed and tested the tools and critically reviewed the final manuscript. Ms. Hodan Abdullah and Ms. Zeinab Idris provided critical review of the final manuscript. Ms. Emelita Jose Ison and Ms. Lamiaa Saleh served as quality improvement coaches. Dr. Saad Jobran, Dr. Hiba Eltahir, Dr. Sair Ibrahim, and Dr. Alaa Khalafalla were involved in reviewing and testing the data collection tools as well as data collection processes. Azza Hassan reviewed and tested the tools and served as an expert reviewer.
Funding
This project was not funded by any organization. The authors declare that there is no conflict of interest.
Conflicts Of Interest Disclosure
The authors declare that there is no conflict of interest.
Informed Consent
Obtained.
Ethics Approval
All methods were carried out in accordance with relevant regulations of the quality improvement department at NCCCR under HMC. verbal consent and voluntary participation in answering the four questions of the tool to participate was obtained from all subjects and/or their legal guardians.
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance And Peer Review
Not commissioned; externally double-blind peer reviewed.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data Sharing Statement
No additional data are available.
Acknowledgements
We would like to express our sincere gratitude to the leaders and palliative care team at the National Center of Cancer care and Research for their valuable support and guidance during this quality project.
References
- Watt C, Scott M, Webber C. Delirium screening tools validated in the context of palliative care: A systematic review. Palliative Medicine. 2021 Apr;35(4):683-96. PMID:33588640 doi:10.1177/0269216321994730
- Fayers P, Hjermstad M, Ranhoff A. Which mini-mental state exam items can be used to screen for delirium and cognitive impairment? Journal of Pain and Symptom Management. 2005 Jul 1;30(1):41-50. PMID:16043006 doi:10.1016/j.jpainsymman.2005.05.001
- Hosie A, Agar M, Lobb E. Improving delirium recognition and assessment for people receiving inpatient palliative care: a mixed methods meta-synthesis. International Journal of Nursing Studies. 2017;75:123-129. PMID:28783489 doi:10.1016/j.ijnurstu.2017.07.007
- Recchia A, Rizzi B, Favero A. Prevalence of Delirium in End-of-Life Palliative Care Patients: An Observational Study. Medical Principles and Practice. 2022;31(2):118-24. PMID:35038708 doi:10.1159/000521994
- Folstein M, Folstein S, McHugh P. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. Journal of psychiatric research. 1975 Nov 1;12(3):189-98. PMID:1202204 doi:10.1016/0022-3956(75)90026-6
- Robinson J. Cognitive assessment of palliative care patients. Progress in Palliative Care. 1999 Jan 1;7(6):291-8. doi:10.1080/09699260.1999.11746854
- Hjermstad M, Loge J, Kaasa S. Methods for assessment of cognitive failure and delirium in palliative care patients: implications for practice and research. Palliative Medicine. 2004 Sep;18(6):494-506. PMID:15453620 doi:10.1191/0269216304pm920oa
- Devenney E, Hodges J. The mini-mental state examination: pitfalls and limitations. Practical Neurology. 2017 Feb 1;17(1):79-80. PMID:27903765 doi:10.1136/practneurol-2016-001520
- Monroe T, Carter M. Using the Folstein Mini Mental State Exam (MMSE) to explore methodological issues in cognitive aging research. European Journal of Ageing. 2012 Sep;9:265-74. PMID:28804426 doi:10.1007/s10433-012-0234-8
- Mudge A, Lee-Steere K, Treleaven E. Cognitive impairment in older hospital inpatients: prevalence, care needs and carer perceptions. Australian Health Review. 2021;46(2):244-250. PMID:34856117 doi:10.1071/AH20286
- Lees R, Corbet S, Johnston C. Test Accuracy of Short Screening Tests for Diagnosis of Delirium or Cognitive Impairment in an Acute Stroke Unit Setting. Stroke. 2013;44(11):3078-3083. PMID:23988641 doi:10.1161/STROKEAHA.113.001724
- Arnold E, Finucane A, Spiller J. Validation of the 4AT tool for delirium assessment in specialist palliative care settings: protocol of a prospective diagnostic test accuracy study. AMRC Open Research [Internet]. 2021 Apr 26;3:16. PMID:35966135 doi:10.12688/amrcopenres.12973.1
- Tieges Z, Lowrey J, MacLullich A. What delirium detection tools are used in routine clinical practice in the United Kingdom? Survey results from 91% of acute healthcare organisations. European Geriatric Medicine. 2021 Dec;12(6):1293-8. PMID:34008099 doi:10.1007/s41999-021-00507-2
- Baird L, Spiller J. A quality improvement approach to cognitive assessment on hospice admission: could we use the 4AT or Short CAM? BMJ Open Quality [Internet]. 2017 Aug;6(2):e000153. PMID:28959786 doi:10.1136/bmjoq-2017-000153
- Shenkin S, Fox C, Godfrey M. Protocol for validation of the 4AT, a rapid screening tool for delirium: a multicentre prospective diagnostic test accuracy study. BMJ open. 2018 Feb 1;8(2):e015572. PMID:29440152 doi:10.1136/bmjopen-2016-015572
- Bellelli G, Morandi A, Davis D. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people. Age and Ageing [Internet]. 2014 Mar 2;43(4):496-502. PMID:24590568 doi:10.1093/ageing/afu021
- Kuladee S, Prachason T. Development and validation of the Thai version of the 4 ‘A’s Test for delirium screening in hospitalized elderly patients with acute medical illnesses. Neuropsychiatric Disease and Treatment. 2016 Feb 24;12:437-43. PMID:26966365 doi:10.2147/NDT.S97228
- De J, Wand A, Smerdely P. Validating the 4A’s test in screening for delirium in a culturally diverse geriatric inpatient population. International Journal of Geriatric Psychiatry. 2017 Dec;32(12):1322-9. PMID:27766672 doi:10.1002/gps.4615
- Evensen S, Hylen Ranhoff A, Lydersen S. The delirium screening tool 4AT in routine clinical practice: prediction of mortality, sensitivity and specificity. European Geriatric Medicine. 2021 Aug;12:793-800. PMID:33813725 doi:10.1007/s41999-021-00489-1
- Hasegawa T, Seo T, Kubota Y. Reliability and validity of the Japanese version of the 4A’s Test for delirium screening in the elderly patient. Asian Journal of Psychiatry. 2022 Jan 1;67:102918. PMID:34798384 doi:10.1016/j.ajp.2021.102918
 This work is licensed under a
This work is licensed under a 